







2023/05/08
2021/04/08
Visit this website for a mentorship programme for children with eye conditions.
2021/02/24
In recent months we have received several reports from patients who had flare-ups of the conjunctiva which has at times led to infection from repeated touching of eyes after sanitization.
Wash hands and eye thoroughly before handling prosthesis. If you experience a flare-up use a good eye drop such as Xailin or Celluvisc. If it does not clear visit your optometrist or ophthalmologist.
2019/09/23
2019/09/23
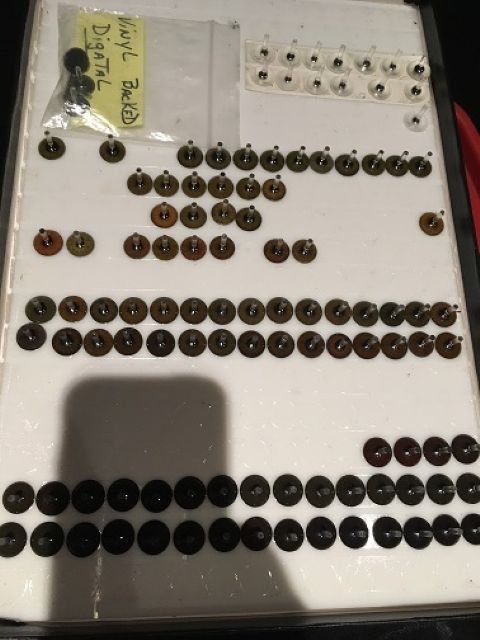
Digital Iris Colours - the latest and the greatest "photo imaging" of the iris (colour) creates a sensational realistic appearance to the Ocular Prosthesis.
Another enhancement we are using is to create a pupil which appears to enlarge as the light is dimmed.
Please come in and consult with Danie or Vida regarding this latest development.
2017/10/18
Good news for our Windhoek Namibian patients!
As from July 2016, we have opened a laboratory and consulting rooms at the Olympia Eye and Laser Centre.
The physical address is: 17 David Carstens Street, Olympia, Windhoek, Namibia.
GPS: 22°36'24.4"S 17°05'53.1"E
Our next visit is scheduled will be announced once we have the all clear to travel internationally.
To make an appointment, please call +27 21 945 4926
2017/10/18
Just a reminder, we have premises in Port Elizabeth.
Should you wish to make an appointment, please contact us on 021 945 4926
The next PE visit is scheduled for Tuesday 21st July 2020 - Thursday 23rd July 2020.
2016/11/17
The ASO (American Society of Ocularsits) Annual Conference held in Chicago this year, October 2016, covered topics such as Surgical Correction of Enophthalmos, by Thomas Johnson, MD, Medical Advisory Seminar, discussion on benefits of Therapy animals in a medical setting, signs of Orbital recurrence of Ocular Tumors Post- Enucleation – a must for any Ocularist, management of floppy eyelid syndrome in the Anophthalmic Patient, Implant Pegging, friend or foe and Subluxed and Extruding Orbital Implants to name only a few.
Highlights were of course given by Randy Trawnik and Dr James Merritt on Fitting techniques for Congenital Anophthalmos and Microphthalmos and Surgical Correction of the Micro-orbit. Insight on a more defined glossary of terms was given when referring to the catch all term – “Clinical Anophthalmia”.
Another highlight was the joint Scientific Session with the AAO. This is where Ocularists and Ophthalmologists have the opportunity of sharing their concerns to obtain more insight into each profession regarding socket (and eye where phthysical eye or microphthalmia is involved) management. The concensus is that a young patient MUST be seen ASAP post enucleation for the fitting of a conformer and ocular prosthesis to avoid contraction of socket and fornices. Also, that aggressive –type expanders are not the preferred choice for children born with micro-orbitism and anophthalmos. A gradual expansion method is far more successful in obtaining soft tissue expansion.
More on a local note, please take a look at a personal account and story of a patient who lost an eye on our Facebook page, “The loss of an Eye: Count your Blessings” Testimonials with photos are also found on our Facebook page.
Support groups are often requested for those recently involved in trauma or Anophthalmos of any sort. If you are able to help these patients/parents deal with this traumatic experience, please contact us via E-mail: vidat_recept@iafrica.com.
2016/01/14
ASO Mid Year Conference 2015
Was held in Phoenix Arizona, USA and abstracts by Dr Zachary Berbos and Dr Ali Ghafouri proved most interesting.
Dr Berbos presented an overview of ocular and orbital embryological development in the human. In addition, common abnormalities resulting from embryologic maldevelopment was discussed. Conditions such as Peters Anomaly which we see at our practice from time to time was discussed.
Dr Ali Ghafouri, MD ,Oculoplastic surgeon, provided an overview of the anatomy, physiology and common pathologies of the nasolacrimal system. Clinical anatomy of the nasolacrimal apparatus as it relates to facial and sinus structures will be discussed. Lacrimal pump mechanism, secretory and out-flow components of the lacrimal system was described. There was a review of common infectious, inflammatory and involutional conditions affecting the lacrimal system. The course covered the medical and surgical management of the dysfunctional nasolacrimal system. We have seen problems occurring from an ill fitting prosthesis regarding the tear secretions in the past.
More technical courses were delivered wrt colour theory and workshops, wear and care of prostheses – are our patients properly instructed and are the instructions followed and retained? Depending on the situation, frequent insertion and removal is not recommended due to loosing the biofilm, an enzymatic or protein film that coats the prosthesis and allows it to be chemically compatible with the anophthalmic socket. Each patient is to be assessed and advised. Likewise, when the prosthesis is polished, is it properly washed before re-insertion? The polish residue can cause a lot of irritation.
Artifical tears are needed by some patients and various types are available, low viscosity such as refresh drops, medium viscosity such as refresh liquigel, high viscosity such as Strauss oil drops (we have in stock) and very high viscosity such as Xailin gel or duratears. Personal preference is important but in dry, dusty areas with lots of wind, careful consideration should be taken as to avoid dye eye problems – in an anophthalmic socket this often results in giant papillary conjunctivitis.
Over and above, fitting techniques were discussed, a gem of a lecture to all Ocularists, young and old.
We take careful note of incorporating all this information, some new and some in the form of reminders here at our practice. This is the only way we believe, of staying on the cutting edge and refining techniques and employing and disclosing information to our patients. Anything you may want to know, just ask. Also be assured that the end product for our patients is a culmination of continued learning and research.
2014/11/24
The 2014 Annual Meeting held at the Marriott in Chicago this year was very good in many ways.
The venue was superb and the topics for discussion were vast and most informative. The meeting spanned most of four days and courses included, correction of the Micro-Orbit”, delivered by Dr Christopher Chambers. Dermis fat grafts are used often nowadays and implants are generally not wrapped. At the joint scientific session with the AAO this was re-iterated.
Much was said at the Joint Scientific Session, American Soc of Ocularists with the American Academy of Ophthalmology – “Making a Bad Situation Better: Retinoblastoma and the anophthalmic Socket”
Subjects such as “Blepharoptosis in the Retinoblastoma Patient” and “Socket reconstruction in Retinoblastoma patients by Dr James Merritt was discussed, “Psychological Implications of Enucleation in Young Children “ highlighted importance in counselling not only children at a later age, but parents. And of course lots more.
Digital technology is stepping up too. There were no less than three manufacturers currently, supplying digitally prepared irises. We have been using them from time to time but find the definition is still better with the hand painting technique.
The great thing about getting together with 180 Ocularists from around the globe is that so many case studies are discussed and ideas are exchanged, our service delivery at the end of the becomes honed and improved.
2014/04/13
Exams, lectures, tests, workshops and discussions with some tasty culinary delights thrown in about sums up the four days’ Annual meeting in New Orleans, held on the 15th - 18th November 2013.
Topics covered included Evisceration and Enucleation techniques, PMMA - polymerisation methods, Fitting the Phthisical Globe, Digital irises, and a most interesting discourse by Dr Todd Swick, MD regarding the Non-24 hour Circadian Sleep Disorder, pertaining to the Circadian rhythm disorder, affecting approx 70% pf totally blind individuals with not light perception…..”without the ability to perceive/receive light signals, the master body clock in the SCN cannot be “cued” or synchronised to the 24-hour day” We, as Ocularists can help identify those who are at risk of Non-24 by educating these individuals that Non-24 is a real illness fist described in 1948 and the first case studies in the late 1970’s and that more information from authoritative sources such as Non-24.com is available. A reminder that we offer a unique service at our practice, to help patients choose the correct frame and lenses to enhance the cosmetic aspects pertaining to dissymmetry so often encompassing the Anophthalmic patient. This was also highlighted by Mr Jim Strauss at one of the workshops…USE IT, its free! The following ASO annual meeting in Chicago takes place on the 17th and the 21st of October.2013/11/13
The ASO fall meeting in New Orleans, Louisiana is from the 15th until the 19th of November. Vida, who is an associate member, will be attending many lectures and writing exams in her time there.
Any special requests pertaining to Ocularisty must please be emailed as soon as possible so that she can take advantage of the experienced master Ocularists which will be there. There will be a lot of emphasis on scleral lenses at the meeting, which is of special interest of both Danie and Vida. Another request has been about developmental obstacles in children with congenital anophthalmia and micro-ophthalmia.
2013/06/05
I don’t remember the time my son was born. I know he arrived on the 29 July 2012 and I think it was around 13.15pm but I cannot be sure. I don’t remember how I felt when he was placed in my arms for the very first time. I feel sad about this but as hard as I try I cannot remember. I guess that’s what happens when you are traumatised. What I do remember was that after the doctor gave him to me I immediately noticed his left eye was shut tight whist the other was wide open and I instinctively felt something was wrong. I asked the doctor ‘what’s wrong with his eye’, to which he responded… ‘oh nothing many children are born that way’.. And then the doctor was gone. I stared at my son for what seemed like hours – but I know it was only seconds – and announced to the room ‘there is something wrong.. he looks funny’. I remember one of the nurses responding ‘how can you say that’. I looked at my husband and I knew that he knew. I said to no one in particular ‘I don’t think he has an eye’. It was then that I forced his eyelid open. I did not see another big beautiful blue eye staring back at me. I saw nothing. I looked at my husband and said ‘he doesn’t have an eye’. We stared at each other for what seemed like many minutes but again I am sure it was just seconds. We both started crying. We knew. We knew something was horribly wrong and this was only the beginning. A paediatrician arrived to examine my son. He only took a minute. He came to my bedside and gently said… ‘You know. You know he doesn’t have an eye’. I nodded and the tears would not stop. ‘It’s called anophthalmia and I have never seen a case of this in all my years as a paediatrician’.
Since that day and for the next six months we saw countless doctors and held my son as he underwent test after test. It began with an MRI to determine whether his brain was okay. It was. The MRI also showed that he had severe microphthalmia and not anophthalmia. anophthalmia means that there is no eye and micropthalmia is an abnormally small eye. microphthalmia occurs in approximately 1 in 10,000 live births and anophthalmia affects 1 out of every 100, 000. (For more information about these conditions see www.macs.org.uk and www.anophthalmia.org). His eye is so small that you cannot see it which is why he was initially diagnosed as having anophthalmia.
Following the MRI my son had a scan of his heart and kidneys and at just 10 days old he had what looked like little suckers placed all over his tiny head as a light was turned on and off for over 40 minutes to determine whether he had sight in his right eye. He did. Over the course of 6 months he had three spacers placed into his empty socket to make it expand. The spacers worked so well that his eyelid went from being shut closed tightly to being wide open. It was then that it became real for me. When I looked at him I always focussed on that blank socket. I couldn’t help it. Friend and family said it didn’t matter. I fooled myself into believing it didn’t.
That is until I had to travel. We had to fly to South Africa to see a specialist. It was during these trips that I saw how others saw him. Some recoiled in shock and gasped and others looked away or looked through us. A man that sat next to me on one unforgettable flight firmly told me I should not let my son stick his fingers into his eyes. Many strangers curiously asked what was wrong. Most stared at him until they caught my eye and then they quickly looked away in pity. I am sure they saw pain on my face. Because when I look back although I told the world I was okay I was not. It’s a very painful experience to see the world look at your son that way. You want them to look at his smile and comment on how adorable it is. You want them to ask his age and his name and comment on how much hair he has. You want them to ask you how you are coping as a new exhausted mom. The fact is we communicate though our eyes. A lot of poetry and some of the most clichéd sayings are about the eyes… you know the one… the eyes are the windows to the soul. So it is a pretty big deal actually when your baby is missing one.
And then I met Vida Trumpelman (www.vidat.co.za). Vida is an ocularist in Cape Town South Africa. Frankly to me she is an artist, a magician and a healer. Put simply she makes and fits prosthetic eyes and in January 2013 she gave my son his first. I wish every one of you reading this could have been in that room when she gave him that eye. It’s hard to describe using words. But if I had to I would say it felt as if I had been holding my breath for too long under water and just as my lungs were going to explode from sheer pressure I came up for air and breathed in deeply. Since that day strangers have commented on the beautiful smile my son has, his thick hair and … his big beautiful blue eyes.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}